Midwifery attendance for home births suspended in Gloucestershire: Women Deserve Better

An Open Letter on Staffing,
Skill, and the Erosion of Trust in Maternity Care
When a home-birth service is suspended,
it doesn’t remove women’s legal right to give birth at home
— but it removes the safety net that makes that choice viable for most families.
Women shouldn’t have to choose between birthing where they feel safe
and having skilled, trusted professionals by their side.
This week,
women in Gloucestershire learned that the
home-birth service has once again been suspended due to staffing shortages.
For families who have spent months preparing for a calm,
supported birth at home,
the announcement brings shock,
frustration and grief.
Staff shortages cannot be an excuse for withdrawing support for women’s choice
Every NHS Trust holds a budget for safe staffing levels.
If the service is unsafe due to low numbers,
the question must be asked:
👉 What is happening to that budget?
👉 How is it being used to maintain equity across localities
— including the Forest of Dean?
👉 And why are experienced, independent midwives
not being contracted to fill short-term gaps for booked home births?
Independent Midwives are experts in community and home-birth care.
They already work in partnership with NHS services elsewhere in the UK under the
NHS Standard Contract,
with indemnity covered through CNST.
This approach could maintain access for women,
relieve pressure on hospital staff,
and preserve trust in the system
— at no additional risk or liability.

A different service requires different skills
The Royal College of Midwives’ Great Trust Midwifery Workforce Report (2024)
recognises the importance of skill mix
and the development of new roles such as maternity support workers,
maternity care assistants,
and nursing associates.
These roles can help provide continuity and early labour support alongside registered midwives — if deployed wisely.
But what is often overlooked is that home birth itself is a different service,
requiring a very specific skill set.
Midwives accustomed to labour-ward environments often describe feeling unsafe at home births
— not because they lack professionalism,
but because they’re removed from the tools and systems they know.
There are many anecdotal accounts from across the UK of higher transfer rates
when home and birth centre births and are attended by midwives unfamiliar with community practice.
It’s understandable: without the “button to press” or immediate backup,
a hospital-trained midwife may prefer transfer
— yet this reflects a systemic failure, not an individual one.
If the professionals we trust to protect physiological birth are losing the skills and confidence to support it,
something has gone seriously wrong.
This cannot be allowed to continue.
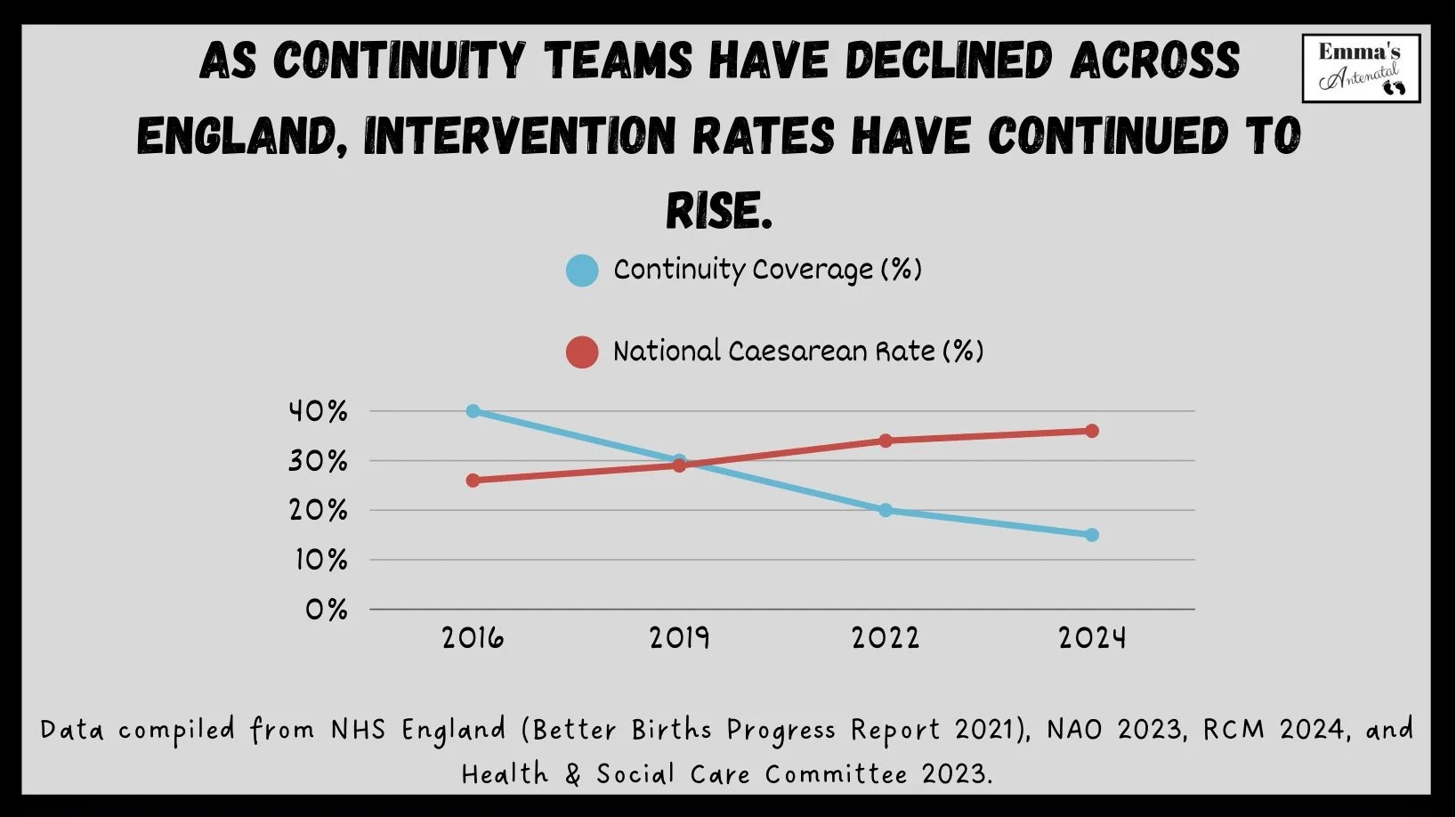
Continuity and confidence go hand in hand
When women have a known midwife,
outcomes improve.
When midwives work in continuity teams, their confidence,
job satisfaction, and retention rates rise.
The Better Births review, the NHS Long Term Plan, and the Cochrane Review (Sandall et al., 2016) all confirm this:
continuity saves lives.
Suspending home-birth and scaling back continuity simultaneously creates a dangerous vacuum
— a system that serves neither women nor midwives well.
Women in the Forest of Dean are being left without maternity services

It is outrageous that an entire district should be left without accessible birth support services:
⛔️ No maternity unit in the new local hospital
⛔️ No promised ultrasound clinic
⛔️ No birth centre
⛔️ No functioning home-birth team
What is happening to the budget allocated for women in the Forest of Dean?
Where is their care, their equity, their right to choose?
This isn’t just a rural inconvenience — it’s a breach of public health duty.
Maternity care should not depend on a postcode.

Rights and Duties
— What the Law Actually Says
It’s important to be clear:
the legal right to give birth at home has NOT been suspended.
Under the NHS Constitution and the Human Rights Act (Article 8),
every woman has the right to decide where she gives birth and who is present.
This includes giving birth at home,
with or without an NHS midwife.
However, as Emma Ashworth of Birthrights notes,
there is no absolute legal right to have a midwife provided to attend a home birth.
The European Court of Human Rights confirmed in Ternovszky v Hungary (2010) that women have the right to choose the circumstances of their birth — including at home — but it did not require governments to guarantee midwifery attendance. In England, the NHS Constitution and national policy (such as Better Births, 2016) set the expectation that home birth should be available, but this is a policy and human-rights obligation, not an individually enforceable statutory right.
What has been withdrawn now, is the NHS midwifery support for home births
— a service that local maternity systems are expected to provide under national policy
(Better Births, 2016) and NICE Guideline CG190.
Integrated Care Boards have a statutory duty under the National Health Service Act 2006 to commission comprehensive maternity services that meet local need,
and the NMC Code requires midwives to support informed choice.
When a Trust repeatedly suspends home-birth attendance,
it risks breaching those duties and undermining women’s human rights to bodily autonomy and family life.
Women can still choose to birth at home,
and emergency ambulance support remains available.
But removing professional midwifery attendance
shifts the responsibility and the risk onto families
— and that is a systemic failure, not an individual choice.
A call to Gloucestershire Maternity Leaders
I call on Gloucestershire’s maternity teams,
LMNS, and commissioners to:
Publish the Equality and Quality Impact Assessments relating to this suspension.
Clarify how safe staffing budgets are being used, and whether underspends are being redirected away from community care.
Explore immediate contracts with Independent Midwives to protect booked home births.
Invest in skill mix — including maternity support workers, maternity care assistants, and nursing associates — to maintain early labour and continuity support.
Prioritise re-establishing continuity models that rebuild trust for women and sustainability for midwives.
We must protect the ability to support normal birth
Home birth is not a luxury.
Let me say that again:
Home birth IS NOT A LUXURY

It is a legitimate,
evidence-based option with strong safety outcomes for healthy women and babies.
The professionals best placed to provide it are those who know the environment,
the physiology, and the families they serve.
If we continue to hollow out these skills,
we risk creating a generation of midwives who no longer feel confident supporting the very essence of normal birth.
This must not be allowed to happen.

Keep reading…
- Add your voice to the comments below
References
Royal College of Midwives (2024). The Great Trust Midwifery Workforce Report.
https://rcm.org.uk/wp-content/uploads/2024/11/0320_GTMWR_section-1.pdf
Section 1: Skill mix and role development (pp. 7–9) – outlines roles for Maternity Support Workers, Maternity Care Assistants, and Nursing Associates in addressing workforce shortages.Sandall, J. et al. (2016). Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database of Systematic Reviews, Issue 4.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004667.pub5/full
Found continuity models reduce preterm birth, intervention, and perinatal loss.Birthplace in England Collaborative Group (2012). Perinatal and maternal outcomes by planned place of birth for healthy women with low risk pregnancies: the Birthplace in England national prospective cohort study. BMJ, 343:d7400.
https://www.bmj.com/content/343/bmj.d7400
Planned home births for low-risk women are as safe as midwife-led units and most cost-effective.**NHS England (2016). Better Births: Improving outcomes of maternity services in England – A Five Year Forward View for maternity care. **
https://www.england.nhs.uk/wp-content/uploads/2016/02/national-maternity-review-report.pdf
National policy advocating continuity of carer and personalised care.**BMC Pregnancy & Childbirth (2017). Prevalence and factors associated with childbirth-related post-traumatic stress symptoms: a systematic review and meta-analysis. **
https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-017-1568-7
Around one-third of women experience trauma after birth; fragmented care and loss of control are major factors.**NICE (2014, updated 2023). Intrapartum Care for Healthy Women and Babies (CG190). **
https://www.nice.org.uk/guidance/cg190
Confirms home birth and midwife-led settings are safe and appropriate options for most women.
If you are still unsure
about the safety of home birth…
Not that it matters what you think
- it’s about the birthing woman,
what SHE thinks and that she can make HER OWN choices
about HER OWN body, baby and risk level.
She is a functioning human adult after all.
But you can listen to Dr Melanie Jackson Phd with a roundup of the latest research
in the excellent podcast.