
Birth Culture - Maternity Services in the UK Today
Before we dive deeper into hormones, I want to pause and take a look at the wider picture: the birth culture and maternity services we’re living in right now and how we got here.
Because here’s the thing
Some of what you will learn about in this course about normal, physiological birth
might sound very different to what you’ve experienced, seen on TV,
read online, or even heard from well-meaning friends or family.
And there are reasons for that…
The Theme of Our Current Birth Culture?
Medicalisation.

Across the UK, birth has increasingly shifted away from being seen as a normal, physiological event
— something a woman’s body knows how to do —
and instead, it’s often treated like a medical emergency waiting to happen.
Let’s look at some examples:
Caesarean section
rates are over 50% in some hospital units (especially large teaching hospitals)Instrumental births
(forceps, ventouse) are on the rise.Inductions of labour is sky rocketing - around 33% nationally.
Although figures can vary wildly across different units from 19-53%Augmentation of labour
(use of synthetic oxytocic drugs to artificially speed up labour) is also around 33%Lithotomy Position
When a woman is on her back with legs in stirrups - 56%Most women want to breastfeed
— but only a small percentage are still breastfeeding a few weeks after birth
- only 2% of babies at 6 months old are exclusively breastfed in line with WHO recommendations.
But is Medicalisation Safer
and Healthier
for Mothers and Babies?
📊 Stillbirth Rates: A Bigger Picture
We’re often told that all of this monitoring, checking, and intervention is making birth safer.
But here’s something to consider:
Despite rising rates of induction, surgical birth and monitoring,
the UK still has one of the highest stillbirth rates in the developed world.
Here’s how we compare (stillbirths per 1,000 total births):
UK: 4.0
USA: 5.7
France: 3.9
Germany: 2.8
Sweden: 2.4
Norway: 2.6
India (for comparison): 12.2
Source: WHO, NHS Digital, World Bank, Statista (2021–2023)
It raises important questions.
If all this intervention was improving outcomes, shouldn’t we be seeing lower rates by now?
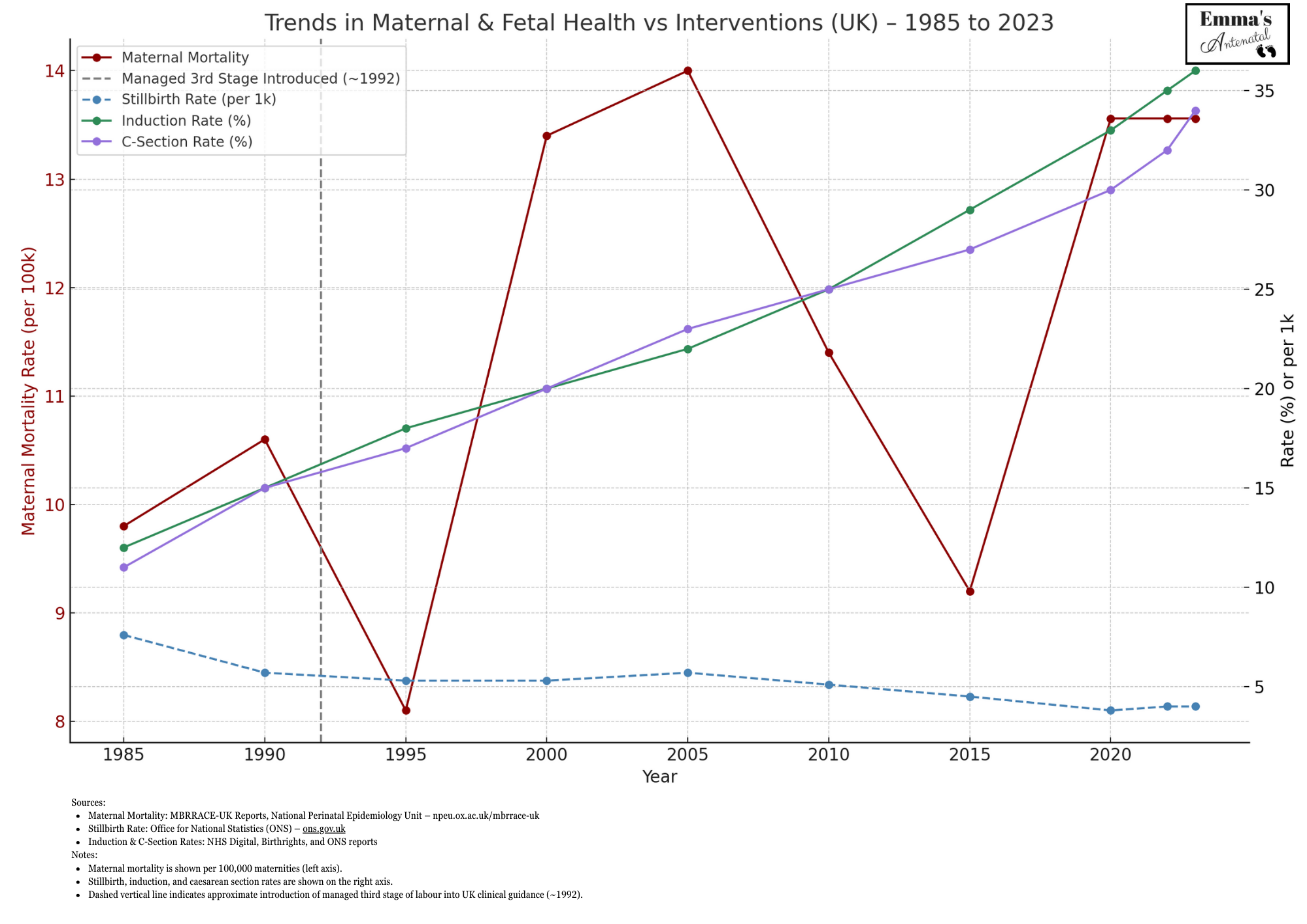
I wanted to go one step further in exploring the link here in the UK between interventions & safety,
so after a bit of digging I’ve come up with this handy visual.
Backstory:
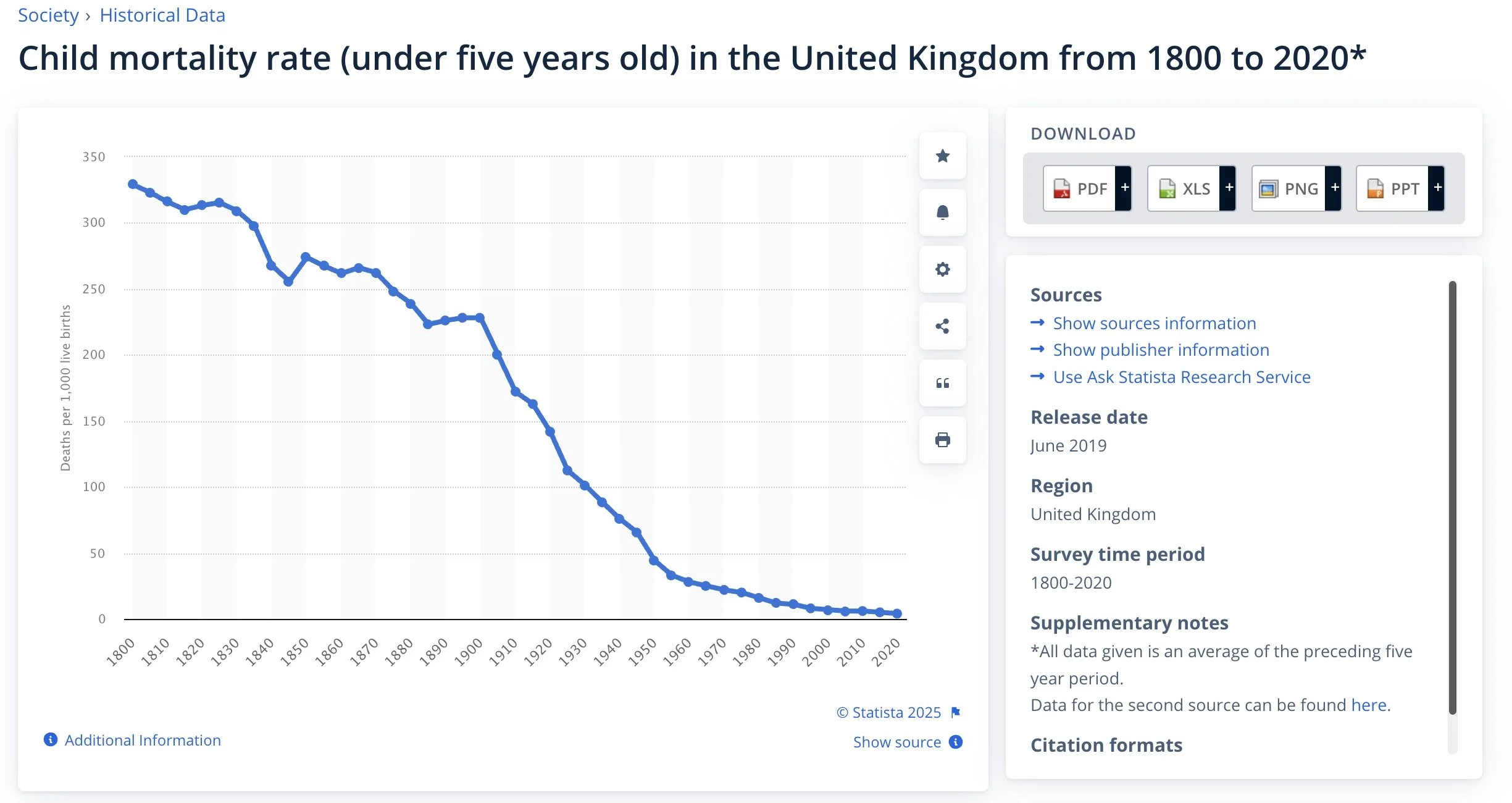
What Happened Before Hospitals?
We often think of hospitals and modern interventions as the obvious answer to safer birth,
after all the maternal mortality and stillbirth rates at the turn of the century were
a few hundred times the numbers today!!
However the story behind why birth is much safer today is more complex,
and worth spending a moment to consider.
Living Conditions
During the 1800’s and early 1900’s, many families in the UK lived in overcrowded, damp, unsanitary housing and were malnourished, suffered with diseases such as rickets, and practices such as corset wearing effected the normal pelvic development.
Higher class women could have been at even greater risk
- living sedentary lifestyles, bound by very tight corsets from their young teenage years.

In UK cities,
it wasn’t unusual for 10 or more people to live in one small room,
sharing an outhouse with 50 others,
with raw sewage seeping into the water supply.
Disease spread easily. Infection was common.
Bathing was rare and hand-washing was not common practice.
This wasn’t about birth being dangerous
— it was about the conditions people were forced to live in.
But how did we end up here?
It’s important to recognise that people did not naturally choose these living conditions,
or end up there through their own lack of ability.
The answer lies further back — in the slow erosion of self-sufficiency.

The Enclosure Acts, passed over centuries,
gradually removed access to common land, and displaced rural families.
People weren’t just "flocking to the cities"
— they were pushed there by loss of land, livelihood, and means to sustain themselves.
Once in the city, they lived in cramped, polluted environments, vulnerable to illness.
Birth along with life in general in these conditions of course became riskier.
Eventually conditions began to improve,
underground plumbing systems were installed,
rivers and wells were cleaned up,
clean drinking water slowly became more available,
houses started to have clean running water,
and indoor bathrooms,
No wonder there were less mothers and babies dying in birth!
and after the 2nd world war as cities were rebuilt
- public health became a priority,
and maternity units were built along with shiny new hospitals
- free healthcare for all with advent of the National Health Service!
Hospitals and interventions had become the solution
- not because birth was inherently unsafe,
but because living conditions had become so degraded.
That’s a very different story
— and it helps us reframe what “safe” really means.
With Woman:
The Evolution—and Erosion—of Midwifery
The word midwife literally means "with woman."
It speaks to something ancient, relational, and deeply intuitive.
For most of human history, birth was supported by other women—trusted companions, wise women of the village, those who had walked the path before.
These were not always formally trained professionals, but they were experienced, present, and emotionally invested.
They came with herbs, knowledge, and time.
Witch Hunts and the Loss of Wise Women
The roots of midwifery were violently disrupted.
During the witch trials across Europe, many of these traditional healers and “gossips”
(originally meaning women who came together to support one another) were persecuted, tortured, and killed.
The trauma of this collective loss still echoes in our cultural memory. It marked a shift from women-led, community-based care to male-dominated control over birth.
Medicalisation and Modern Midwifery
Over the last few centuries, midwives were brought under state and medical authority.
In the UK today, most midwives are trained primarily in obstetric-led settings.
The role has become increasingly medical,
risk-focused,
and protocol-driven.
While many midwives still carry the heart of “being with woman,” the system often prevents them from practising this way.
Caseloading teams
where a woman is supported by a known midwife throughout pregnancy,
birth and postnatally—do exist,
and they’re shown to increase satisfaction, reduce interventions, and promote physiological birth.
But they’re the exception, not the rule.
Most women now experience fragmented care:
Short appointments in a clinical setting rather than in their home
Tick-box interactions
A new face at every visit
No space to build trust
This disjointed model undermines the very conditions that help oxytocin flow:
safety, familiarity, emotional presence.
💔 The Impact on Midwives Themselves
And it’s not just parents affected by this system.
Midwives are working under huge pressure.
Over half report being bullied or undermined at work (RCM, 2016), and it’s often called one of the most bullied professions in the NHS. Many leave the profession, not because they don’t care — but because they can’t offer the care they came into this work to give.
And this really matters.
Because birth hormones don’t just come from the person giving birth — they’re influenced by the emotional atmosphere of the whole room.
If a midwife is rushed, anxious or exhausted, that stress is felt. Hormones like adrenaline and cortisol are contagious. And oxytocin — the hormone we need for labour and bonding — only flows when we feel safe.
So What If Women Went
Back to the Darkened Room?
There’s a well-known story about cats giving birth that says it all.
Everyone knows that when a cat is in labour, she’ll head off to the darkest, furthest room she can find. She needs quiet, darkness, and safety.
But in this story, the scientists want to help her. So they bring her into a bright, sterile lab. But in the lab, she can’t birth easily — she’s in pain. So the scientists invent drugs to help. Over time, the original scientists retire… and the next generation forgets that cats ever gave birth easily in the dark.
And that’s where we are now with birth.
📺 I’ll tell the full version of that story in the next video:
👉 Back to the Darkened Room
🧡 Why This Course Matters
Because when you understand the system you’re giving birth in, you’ll see why supporting your own body’s natural hormones — and knowing how to protect them — is so powerful.
You can create a calm, safe, empowered birth experience, even within a system that doesn’t always prioritise it.
This course is here to show you how.
And whether you’re preparing to give birth, or supporting someone who is, this knowledge matters — for our births, our babies, and our future.
📝 Journal Prompt:
Let’s take a gentle pause to reflect on your experiences (or impressions) of maternity services.
Whether you’ve accessed maternity care yourself, or job is being a part of the system,
have you support someone who has gone through NHS maternity care,
or simply encountered stories from friends, family, or media
— it all shapes how we feel about birth and care systems.
Take a moment to consider:
Have you experienced maternity services firsthand? What stood out to you — positive, challenging, surprising?
Were there moments that felt empowering, or perhaps moments where you felt overlooked?
If you haven’t personally accessed these services, what ideas or feelings come up when you think about maternity care?
Feel free to express your thoughts however feels natural:
✨ Write down reflections, memories, or feelings.
✨ Doodle, sketch, or use color to capture your experience.
✨ Even a single word or phrase is enough.
And, as always, share something in the comments below! 💬
Your perspective might offer comfort, insight, or encouragement to someone else in our community.
Let’s keep the conversation open and supportive.