
Birth: No Place for Ideology
This weekend saw the release of a major Guardian investigation
— a full year of research —
exposing the tragic consequences linked to the Free Birth Society.
And I’ll be honest:
I am shocked.
I am saddened.
And I feel compelled to add my voice.
I’ve spent 18 years studying & researching birth — teaching it,
supporting families through it, studying physiology,
reading the research, diving deep into the legal frameworks,
and witnessing firsthand how maternity systems shape our choices.
I’ve seen the beauty of undisturbed birth,
and I’ve seen the damage caused by an overstretched,
medical system.

So when I read this investigation,
my heart broke, yet again,
it regularly does these days it seems.
— not because of the women seeking autonomy,
no because women are choosing freebirth,
— but because birth ideology has now taken a hold at both extremes,
The only reason
“Freebirth ideology”
could thrive
is because “medical birth ideology” already took hold.
When you have a system where:
women are dismissed or disbelieved,
consent is ignored,
trauma is normalised,
midwife-led care is dismantled,
continuity disappears,
and caesarean rates climb to nearly 50% in some UK hospitals (including Gloucester)…
Women are quite rightly going to start looking for alternatives

A Global Problem…
This isn’t just a UK problem either — far from it.
In fact, we’re one of the last remaining countries where midwife-led care still exists at any meaningful scale and we must do all that we can to hold on to it.
Across the world, birth has become dangerously over-medicalised:
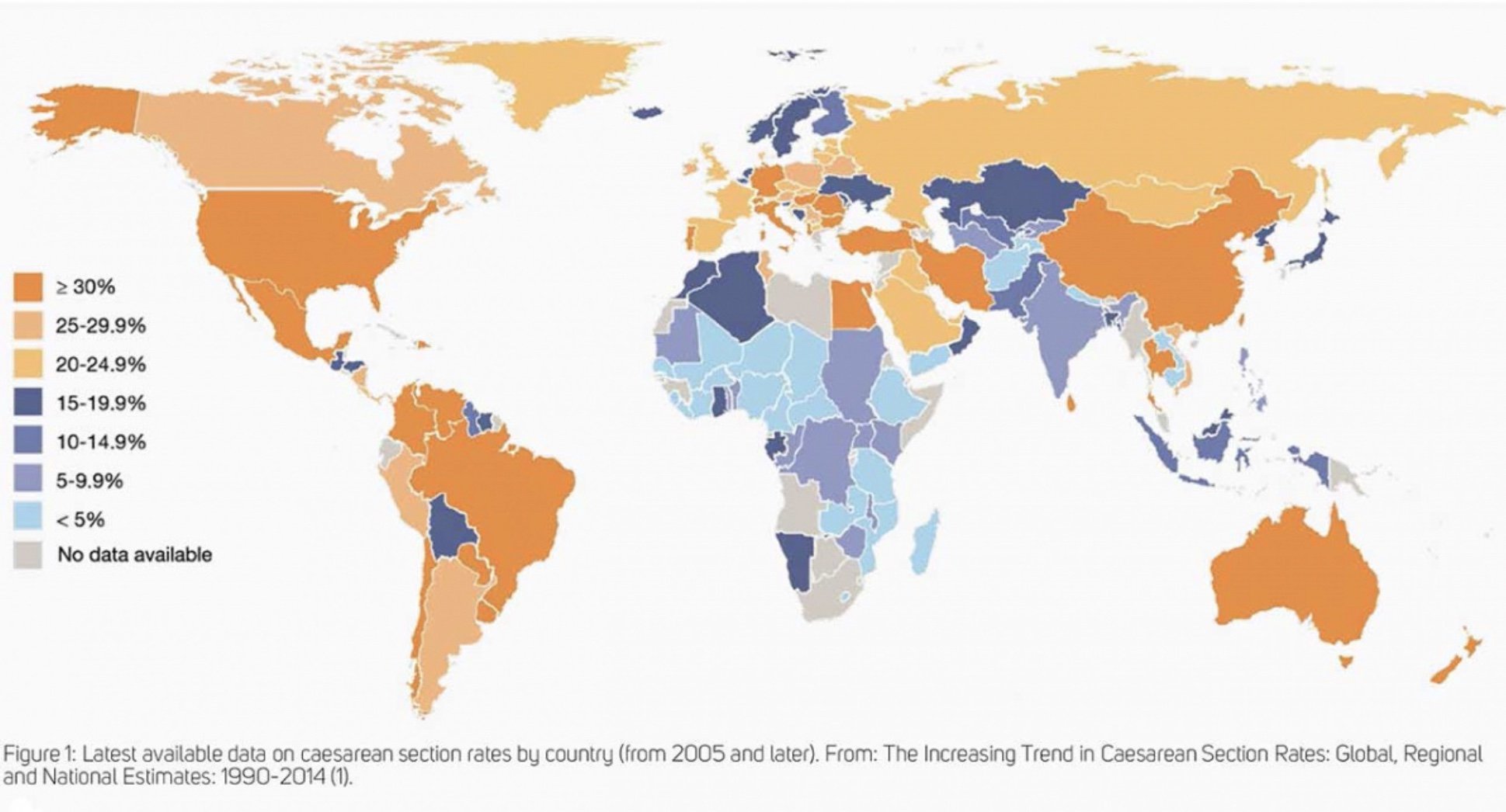
Map showing worldwide data up to 2014, medicalisation had already begun…
United States: epidural rates over 90% in many hospitals;
induction and caesarean rates rising every year; midwife-led birth barely 10% of all births.Brazil: private hospital caesarean rates exceed 90%,
with national rates hovering around 55–60% — one of the highest on Earth.Turkey: caesarean rates now over 60%.
China: historically around 45–50%.
Italy: national caesarean rates around 35–40%,
much higher in private units.India: caesarean rates vary widely,
but some private hospitals exceed 70%.

Contrast this with the World Health Organisation,
which states that population-level caesarean rates above 10–15%
are not associated with increased safety,
and instead signal overuse,
unnecessary risk,
and long-term health consequences for women and babies.
When you zoom out, the pattern is unmistakable:
birth worldwide is being pulled further and further into a surgical, intervention-first model
— even when evidence doesn’t support it.
And when women feel overpowered,
dismissed or harmed by that model,
they naturally look for alternatives.
The problem isn’t that women are rejecting the system.
The problem is that the system has stopped being a safe place for women.
When leadership blames women instead of fixing the system
And while we’re talking about ideology and safety,
let’s address what happened here in Gloucestershire just two weeks ago.
The CEO of Gloucestershire Hospitals stood in front of the Health Scrutiny Committee and said,
quite openly, that women are making “the wrong’ choices based on fear and anxiety from the media.


— and used this as justification for the Trust removing the homebirth service.
Homebirth is an important legal choice.
Trusts have a duty to provide safe staffing for all legally available services.
Trusts have duties around service provision,
and removing a legally available choice
because leadership disagrees with women’s decisions
raises serious legal and ethical concerns.
And then — unbelievably — he stated that midwives need to be “trained” in how to speak to these women, widely interpreted by many of us as implying that midwives should talk women out of homebirth.
He also suggested that media coverage of the Manchester tragedy contributed to their knee-jerk,
fear-based suspension of homebirth
— which many found deeply contradictory,
given that he had also criticised women for making
“fear-based” decisions themselves.
He further expressed disagreement with the large body of evidence supporting homebirth safety.
The evidence for planned homebirth safety is strong and consistent across multiple large population studies.
His comments appeared to completely disregard that body of evidence.
This is the exact mindset that drives women away from the system in the first place.
It is paternalistic, outdated, and misleading.
If we want safer births?
If we want fewer emergencies?
If we want better outcomes?
We don’t achieve that by shutting down choice or retraining midwives to persuade women into hospital.
We achieve it by doing exactly the opposite of what he described.
Just look at Somerset:
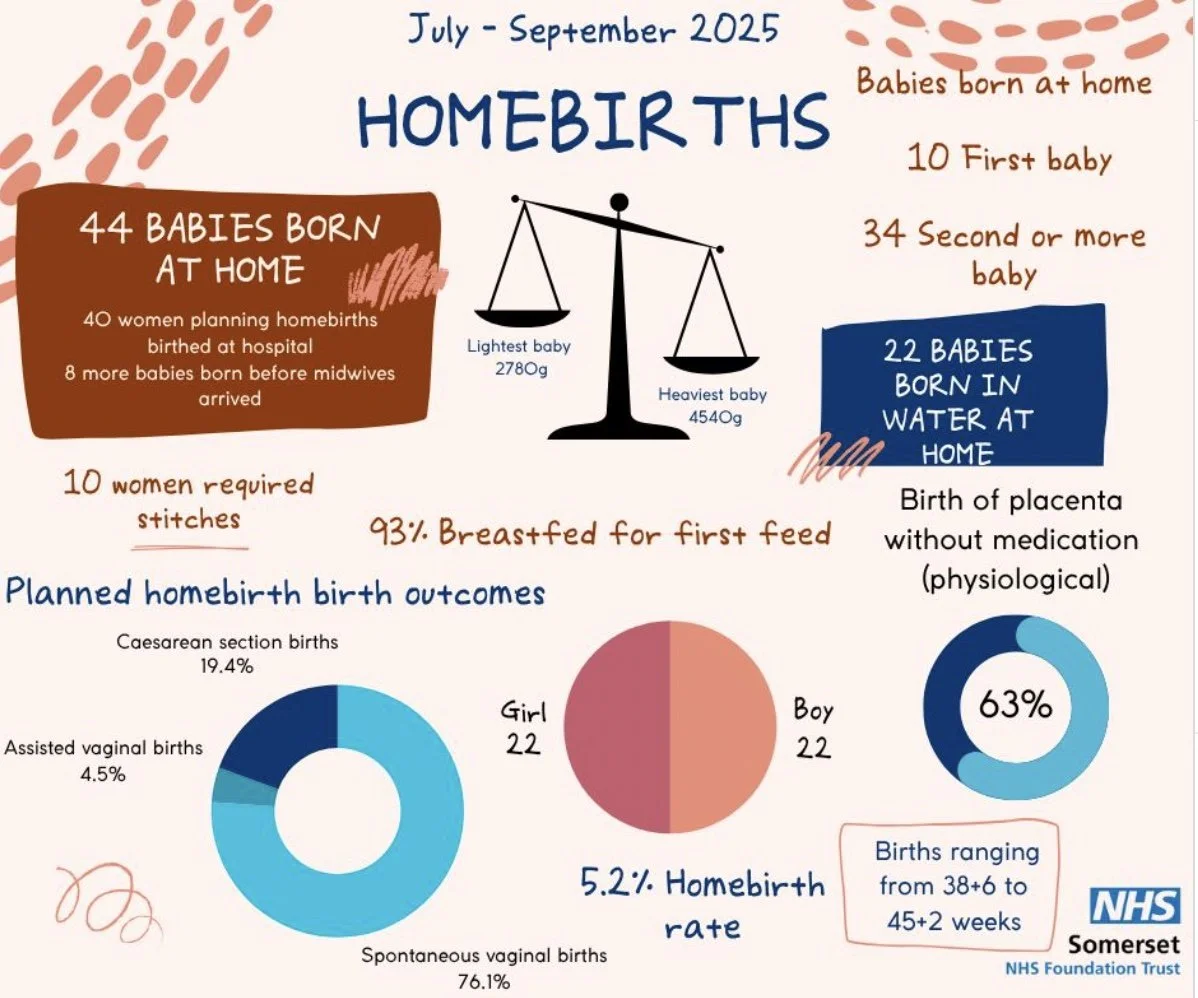
Most were spontaneous vaginal births, with extremely positive outcomes.
This is what care looks more like when it is begins to be supported,
staffed, and trusted.
The more homebirths you support,
the more experienced midwives become.
The more experienced they become, the safer the service becomes.
Safety grows out of investment, continuity, confidence and trust
— not out of removing the service entirely.
And here’s the truth nobody at board level seems willing to admit:
The skills and expertise needed for safe homebirth already exist
— in our community.
Experienced independent midwives are right here.
They are skilled, insured, evidence-based,
and ready to work alongside newly qualified NHS midwives
to pass on the exact knowledge hospitals claim is “missing”.
The fact that they have been ignored
— while women lose their right to homebirth —
is a political choice, not a clinical one.
This is the moment where leadership needs to drop the ego,
stop blaming women, and start embracing the resources already around them.
Because women’s choice is not the problem.
Removing choice is.
Why a subculture turned away from medical care altogether…
A freebirth ideology didn’t arise in a vacuum.
It grew out of iatrogenic harm
— the harm caused by the system.
The birth injury claims paid out by the Trust relate to incidents in obstetric settings,
not homebirths or midwife-led units
Why not ease the pressure on an overstretched obstetric team,
by promoting home birth and midwife-led units to the women who don’t need medical interventions?
The evidence for planned homebirth safety and midwife-led care is strong, consistent,
and supported by multiple large population studies and national guidelines.
Kevin McNamara’s comments appeared to disregard that evidence,
despite its clarity and longstanding inclusion in national policy.

When women are traumatised, denied options, or frightened into procedures, trust shatters.
And into that broken space steps anyone willing to promise sovereignty, safety, and a return to instinct.
But replacing one rigid ideology with another helps no one.
Birth has no place for ideology.
Not the ideology of:
“hospital is always safest”.
Not the ideology of :
“birth is always safe and emergencies are imagined”.
Both erase complexity.
Both create blind spots.
Both put women and babies at risk — just in different ways.
What can we do?
Where evidence and credibility matter….

To navigate between these extremes,
we all need to rely on solid information from credible sources.
Cross reference idea’s with many people, in any chosen field -
in birth look for those with valid qualifications, like myself,
and other qualified Doula’s Midwives and Birth-keepers
look at a wide range of qualified, published authors with integrity, like:
Look at NICE guidance, AIMS, Association of Radical Midwives,
and even the Green Top Guidelines published by the RCOG.
You don’t have to agree with everything
— but knowing the evidence helps you understand your baseline.
And alongside reading research, it’s just as important to read opinion pieces
— the kind that make you think, question, disagree, and grow.
Read Ina May Gaskin, Sheila Kitzinger, Grantly Dick-Read (with a critical lens),
and the historical threads of midwifery wisdom.
Read Milli Hill, Beverley Beech, Leah Hazard, and articles from AIMS,
Birthrights, and the National Childbirth Trust.
Explore commentary from The Conversation, BMJ Opinion,
and even viewpoint pieces from the RCOG and Royal College of Midwives.
Listen to podcasts that explore physiology and humanity from multiple angles
— The Mother of all Podcasts,
The Great Birth Rebellion, Midwifery Hour,
and others who walk the line between evidence and lived experience.
And then — crucially —
challenge yourself to read and listen to things that sit directly opposite your current beliefs:
Amy Tuteur (Skeptical OB),
look for similarities…
Listen to the voices that irritate you,
that you want to switch off,
that trigger something in you.
Ask yourself what part of you reacts, and why.
Ask where the truth might be hiding inside a perspective you instinctively resist.
This is not just good birth research philosophy
— this is good life research philosophy!!!
Being willing to sit with opposing ideas,
to sift truth from ideology,
and to examine your own responses is the foundation of true autonomy.
Because autonomy is not about clinging to one viewpoint.
It’s about having the breadth, maturity and humility to explore all viewpoints
— and then deciding from a grounded place, rather than a reactive one.
And even then?
Evidence does not override your intuition.
It can guide you,
but it cannot replace your embodied sense of what feels right.
Different women,
with different histories and needs,
will make different decisions:
Some choose a planned caesarean — for deeply personal, valid reasons.
Some choose midwife-led home birth.
Some choose freebirth — sometimes through ideology,
often through circumstance,
and very often because they have been denied safe midwifery care.
None of these choices are irresponsible when they are informed, supported, and grounded in reality.
This is why, throughout the pages of my website, you’ll see me reference:
law,
guidance,
clinical evidence,
physiology,
and the real range of outcomes.
I am transparent about what is evidence, what is guidance, what is opinion, and where intuition fits.
Birthwork in the UK, Europe & across the world is not ideology
— it is grounded, rational, rooted in safety,
evidence and listening to women, not telling them what to do.
It’s crucial to say this clearly:
Birth-keepers, doulas and educators in the UK and across the World
operate from an entirely different foundation than extreme ideology.
We take pride in:
woman centred care
evidence literacy
trauma-informed support
legal awareness
collaboration with midwives
supporting women’s instincts and safety
recognising red flags early
supporting hospital transfer
helping women to plan, prepare, and support self-monitoring
We are not pushing an idea.
We are supporting informed decision making.
Nobody can ever promise 100% safety.
We look at risks vs benefits.
We are not romanticising physiology.
The birth community here is overwhelmingly:
reasonable
rational
grounded
safe
collaborative
and committed to women’s autonomy with real-world support
Most UK women who choose to freebirth are doing so with:
careful planning
awareness of warning signs
readiness to seek help
and often because of previous trauma, or because safe midwifery services have been withdrawn,
not because women believe birth emergencies are imaginary.
This is why it’s essential we don’t allow the actions extremist subculture to overshadow the thoughtful,
responsible, evidence-guided birthwork happening here.
Birth deserves respect, clarity,
autonomy and truth — not dogma.
Whether a woman births by caesarean, at home with midwives, or unassisted —
her choice is not just valid.
It is her human right
My commitment is simple:
to keep offering evidence, nuance, honesty and support
— so women can make decisions that are truly theirs.
Birth should not be battleground for belief systems.
Birth is human, physical, emotional, embodied, and deeply individual.
And it deserves better than ideology
— from any direction.

About the Author & Ongoing Advocacy
Emma Gleave has spent nearly two decades researching birth, supporting families, and advocating for safe, evidence-based maternity care. Her recent work includes detailed FOI investigations, analysis of local maternity policy, and public advocacy around the suspension of homebirth services in Gloucestershire, UK.
She documents this work openly so women, families and professionals can follow what’s happening and stay informed. You can read more and keep up to date with her ongoing advocacy on her website..