
Gloucestershire’s New Community Birth Plan — What We Know So Far

Recently we have heard that Gloucestershire maternity services are introducing a new model for out-of-hospital birth cover.
The proposal appears to involve a small pool of midwives on call to cover:
Stroud Midwife-Led Unit
Cheltenham Birth Centre
Home births across the county
We believe this model may already be operating, although clear communication from Gloucestershire Hospitals NHS Trust has been limited, making it difficult for families and professionals to understand what is actually happening.
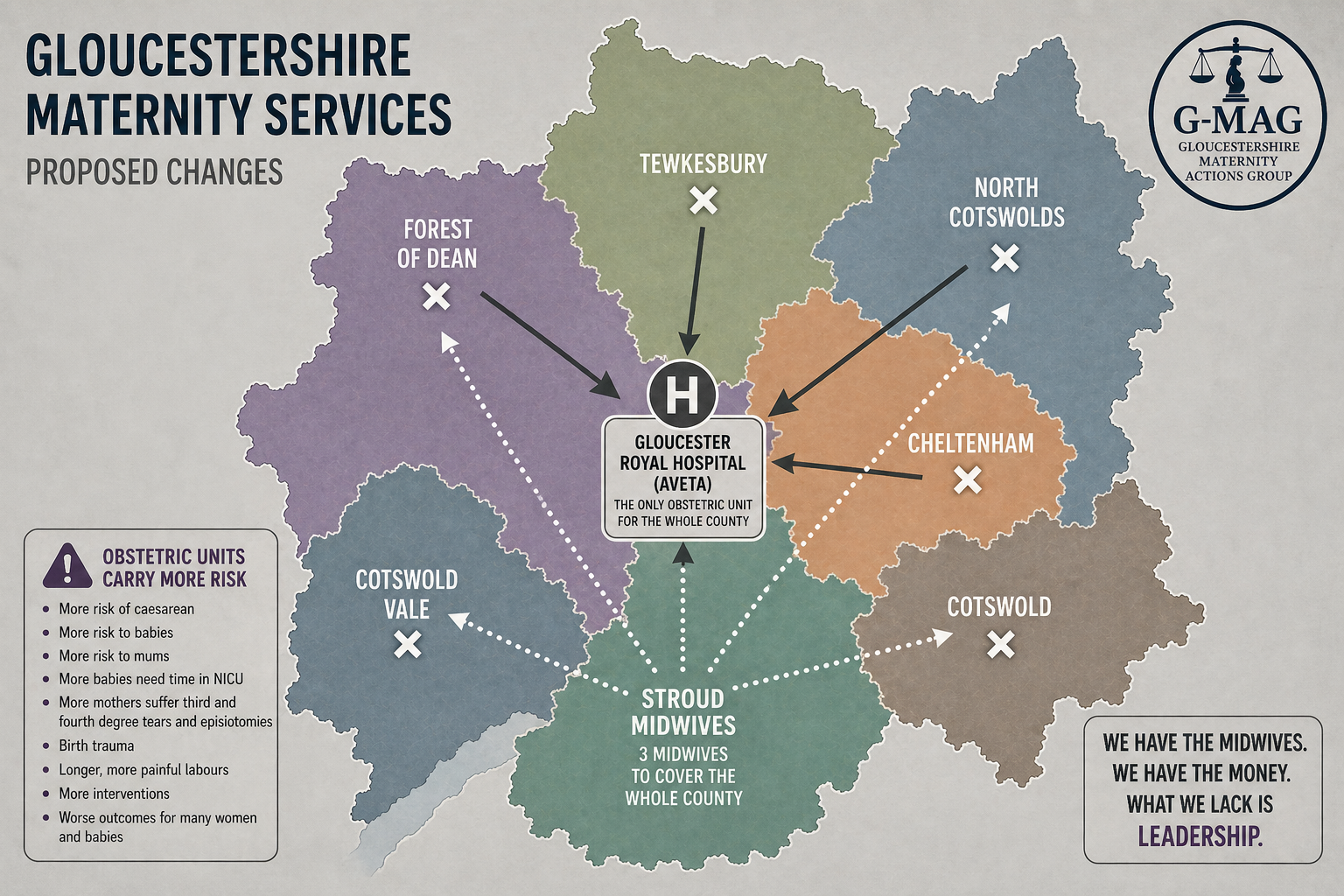
What we have been told suggests that three or possibly four midwives will be on shift at any one time.
Because two midwives are required to attend every birth, this would mean that:
Only one out-of-hospital birth could be staffed at any one time.
If two women went into labour simultaneously in the community — for example one planning a home birth and another at Cheltenham Birth Centre — one of them would need to be redirected to Gloucester Hospital.
There is still no clear public explanation of how this system will work in practice.
The Scale of Birth in Gloucestershire
Gloucestershire sees around 6,000 births per year, which works out to approximately:
500 births per month
115 births per week
16–17 births per day
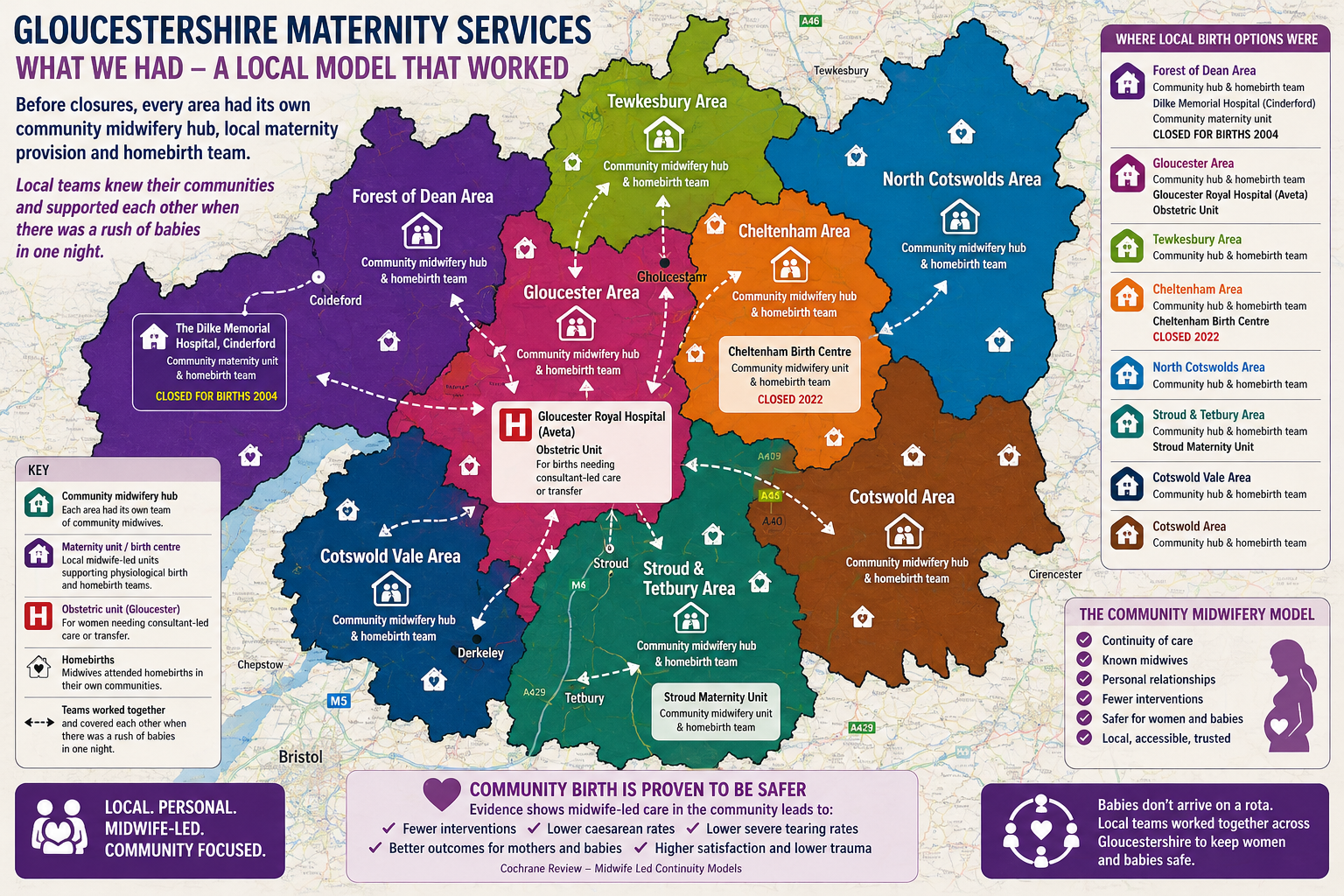
Community birth settings historically accounted for a small but important proportion of those births.
Based on recent figures:
Stroud Maternity Unit: around 300 births per year
Cheltenham Birth Centre: around 16 births per month before its closure in 2022
Home births: approximately 4–6 per month before the recent suspension
Taken together, this represents roughly 46 births per month in community settings.
Under the proposed staffing model, it is likely that a significant proportion of these births could not be attended by midwives, simply because the service would only be able to support one out-of-hospital birth at a time.
This raises serious concerns about what happens when more than one woman goes into labour.
Would women be:
redirected to hospital against their wishes?
asked to change their birth plan late in pregnancy?
or potentially left without the midwife-led care they had planned?
For many families, this effectively means choice exists on paper but not in practice.
The Changing Needs of Women
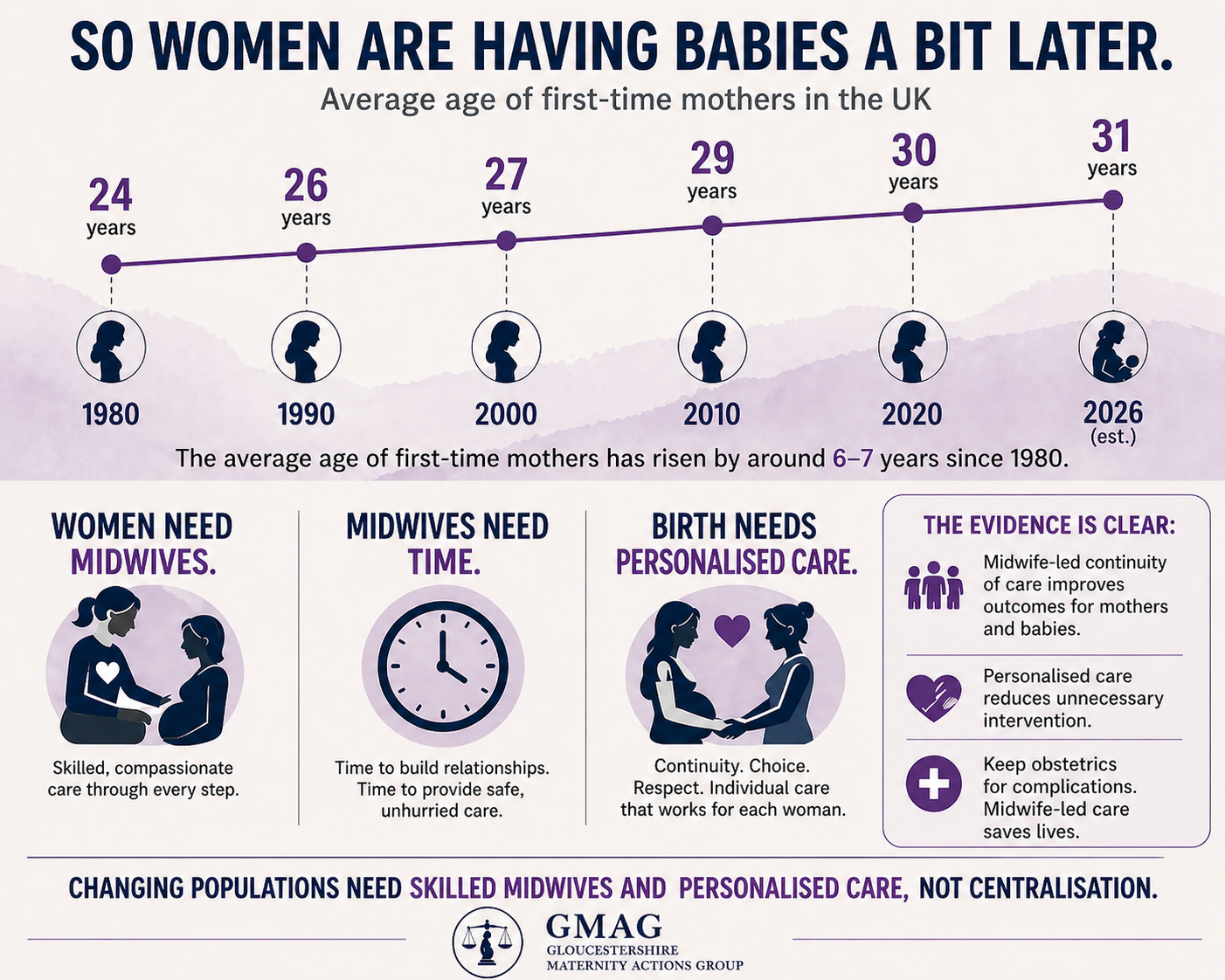
We are also repeatedly told that these changes are being made in response to the “changing needs of women” and that the Trust is taking an “evidence-based approach.” But this framing is deeply misleading.
What has changed in many cases is not women’s needs, but the demographic profile and medical classification of the childbearing population.
Women may be slightly older when they have their first baby, or have a higher average BMI than in previous decades, but these factors alone do not automatically mean that obstetric-led care is safer or necessary.
There is no clear evidence that directing larger numbers of women into highly medicalised, obstetric-led environments improves outcomes.
In fact, research consistently shows that midwife-led continuity models reduce intervention and improve experiences for women and babies.
When maternity systems respond to demographic shifts by expanding risk labelling and centralising care, rather than strengthening community midwifery and continuity, women are effectively pushed toward intervention-heavy pathways.
The result is a system where decisions about what women supposedly “need” are imposed from above, often justified through fear-based narratives about risk rather than genuine evidence of improved outcomes.
What About Community Midwives?
Another question that remains unanswered is who exactly is expected to staff this model.
Are midwives from Stroud expected to cover Cheltenham Birth Centre as well as all home births across the whole county?
And what role will local community midwives in areas like the Forest of Dean or Cheltenham play?
Many community midwives currently focus almost entirely on antenatal and postnatal care, rarely attending births.
If that is the case, there is an obvious opportunity being missed.
Rather than stretching a small on-call team across the whole county, Gloucestershire could invest in re-skilling community midwives in home birth and midwife-led birth centre care.
There are independent midwives, registered with the NMC and safe to practice as skilled professionals, who are ready to assist with homebirths and the reskilling / upskilling of NHS midwifery colleagues.
Continuity of Care Is the Safest Model

The safest maternity systems are built around continuity of care,
where women know the midwives who support them during pregnancy and birth.
When women feel safe with skilled midwives they know and trust, their birth choices often change dramatically.
In continuity and caseload models around the world, home birth rates have ranged anywhere from around 20% to as high as 80%, depending on the model.
This is not about pushing women towards home birth.
It is about ensuring women receive balanced information, skilled care,
and genuine choice throughout pregnancy.
Too often in fragmented systems, women are subtly conditioned to believe their bodies are fragile or dangerous — that birth must be closely controlled by technology and intervention.
Continuity models instead recognise that birth works best when women feel safe, supported and respected.
This is the essence of midwifery: with-woman care.
The Hidden Cost of Intervention

When women are directed into busy obstetric units rather than supported in midwife-led environments, intervention rates increase.
These settings are associated with:
higher use of epidural analgesia
increased likelihood of instrumental birth
higher rates of caesarean section
increased risk of severe perineal trauma
Women are also more likely to report traumatic experiences of care when they are supported by unfamiliar staff in high-pressure clinical environments.
These harms are not just emotional — they are also financial.
Maternity claims represent the largest single cost area for NHS clinical negligence, accounting for more than half of the total value of claims each year.
Improving continuity of care and reducing unnecessary intervention is not only safer for families — it also reduces long-term costs for the health system.
Women Deserve Clear Answers
At present, there are still many unanswered questions.
Is this model already in operation?
Have postnatal beds been removed?
How many midwives are actually on shift — three or four?
Who will cover home births across the county?
What role will community midwives play in intrapartum care?
How will genuine choice for women be protected?
Families in Gloucestershire deserve clear communication and transparency about the future of their maternity services.
Because maternity care is not simply about managing risk.
It is about supporting women through one of the most important events of their lives with safety, dignity and skilled care from professionals they know and trust.
Money in the Bank
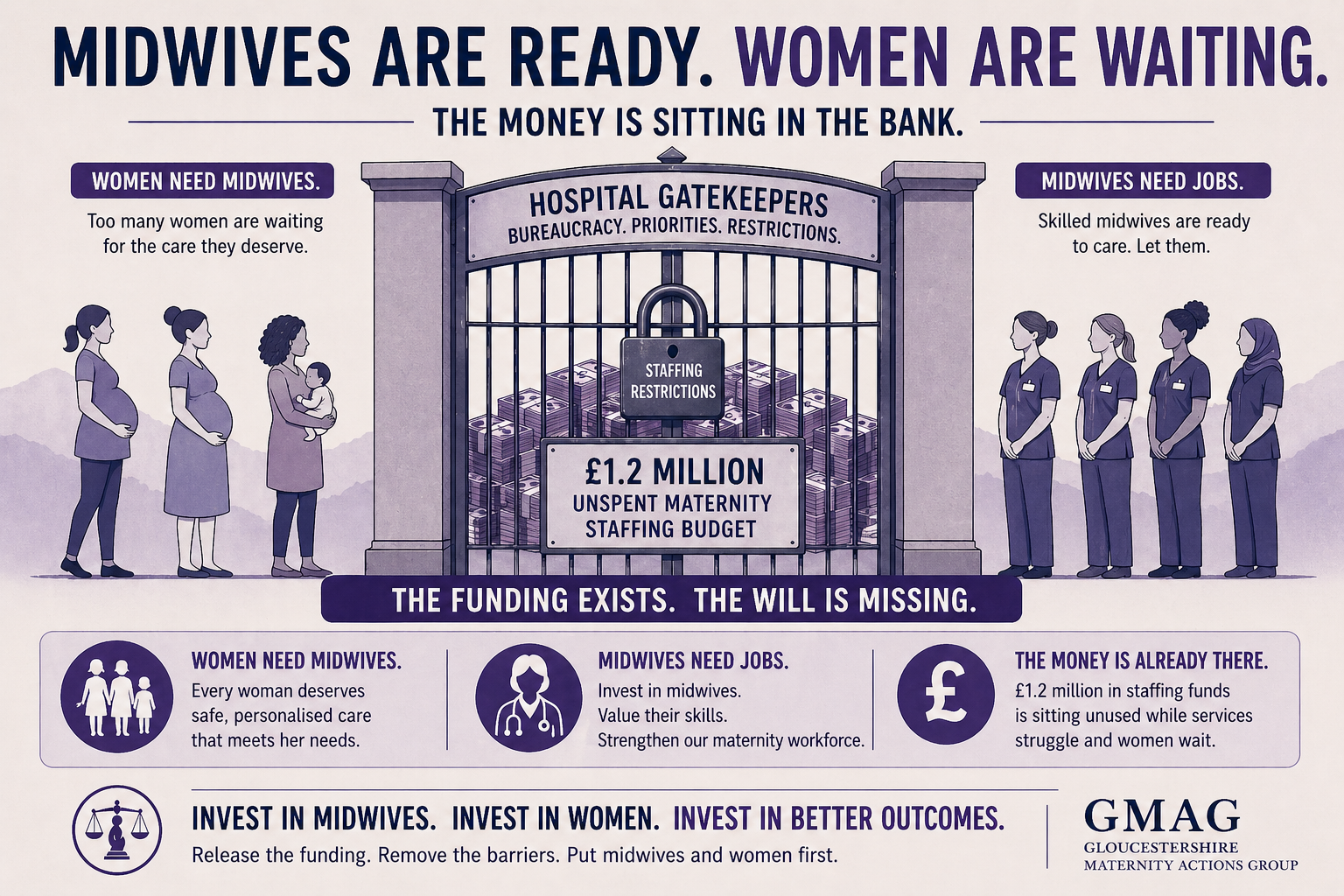
Through Freedom of Information requests, we now know that Gloucestershire Hospitals NHS Trust has around £1.2 million in unspent staffing budget.
At the same time, newly qualified midwives are struggling to find employment, experienced community midwives are being pulled away from the work they trained to do, and women across the county are being told there are “not enough midwives” to safely support homebirths or midwife-led units.
The contradiction is stark.
There is money allocated for staff that is not being used, midwives who need jobs and experience, and women who need skilled midwives to support them in pregnancy and birth.
In addition, Gloucestershire has a strong presence of independent midwives, many of whom are highly experienced and willing to collaborate with NHS teams—supporting services, mentoring younger midwives, and helping rebuild skills in community and homebirth care.
Instead of using these resources, services continue to be withdrawn.
Birth centres remain closed, homebirth services suspended, and community midwives deskilled by systems that rarely allow them to attend births.
With funding available and skilled professionals ready to work, the continued restriction of community birth options is difficult to justify.
At a time when both midwives and women need support, leaving this money unused while services disappear feels like the very definition of irrational policy and incompetent leadership.
Where Is the Accountability?

Major changes to maternity services should not happen quietly or by rumour.
When services that families rely on are reduced or fundamentally altered, there should be clear communication, public explanation, consultation and proper scrutiny.
So far, many of the key details surrounding this proposed model remain unclear. Families, midwives and campaign groups are still asking basic questions about how the service will operate and who will staff it.
If community birth is effectively limited to one out-of-hospital birth at a time across the county, that represents a significant restriction on maternity choices for Gloucestershire women.
Decisions of this scale should involve:
transparent communication from the Trust
proper scrutiny by the Integrated Care Board
oversight from the Health and Care Scrutiny Committee
and genuine engagement with the women and families who use the service
Instead, many people feel they are piecing together information through conversations and fragments rather than clear public statements.
Women deserve better than uncertainty when planning where and how to give birth.
Maternity services should be built around evidence, safety and genuine choice — not systems that quietly make certain options impossible in practice.
Until Gloucestershire Hospitals NHS Trust provides a clear explanation of this model, serious concerns remain about whether community birth in the county is being restored in any meaningful way, or simply reduced by another name.