
Rethinking Safety in Maternity Care: Beyond the Banding
Time for a Skills Matrix?

Across the UK maternity system, discussions about safety often focus on staffing numbers, service configuration, or the location of birth. Yet one of the most overlooked issues is how midwifery skills are structured and maintained within the system itself.
Current workforce models often assume that midwives are interchangeable across all maternity settings. In reality, midwives develop specialist expertise depending on the environments in which they practise.
Recognising this reality could strengthen safety, professional confidence and workforce sustainability.
One practical step forward would be the introduction of a national midwifery skills matrix,
used alongside the existing banding structure,
to recognise and maintain the wide range of competencies midwives develop throughout their careers.
What do you think
- is this a better way forwards?

Why the NHS Banding System Does Not Reflect Midwifery Skills

In the NHS, midwives are organised according to the ‘Agenda for Change’ banding structure.
These bands are primarily designed to reflect seniority, responsibility and time in post,
rather than the specific clinical environments in which midwives practise.
A Band 5 midwife is newly qualified
Band 6 midwives typically take on greater clinical responsibility.
Band 7 roles often include leadership or management duties.
However, banding does not necessarily reflect experience across different birth settings.
A Band 5 midwife may have recently completed extensive placements supporting physiological births and home births during her training.
She may feel confident attending births in community settings.
Meanwhile, a Band 7 midwife who has worked exclusively on a labour ward for several years may have significant leadership experience but may not feel confident attending a home birth if she has not practised in that environment for some time.
Both midwives are highly skilled professionals
— but their expertise lies in different areas of practice.
The banding system therefore cannot be used as a reliable measure of whether a midwife is experienced in a particular birth environment.
Recognising and documenting actual clinical experience,
rather than relying solely on job banding,
would allow maternity services to better understand the expertise within their workforce.
Experience Should Match the Birth Environment

A common response to discussions about midwifery skills is the suggestion that newly qualified midwives should spend a period of time working on labour wards before moving into community or home birth practice.
However, this assumption deserves careful scrutiny.
Labour wards are designed to support women who require obstetric care.
They involve continuous monitoring, medical interventions and multidisciplinary escalation protocols.
These are important skills
— but they are not the same skills required to support physiological birth in community environments.
Home birth and birth centre midwifery
require confidence in:
supporting undisturbed labour
recognising subtle early deviations from normal physiology
autonomous clinical judgement
neonatal resuscitation without immediate medical backup
These skills are best developed through experience in physiological birth settings,
not through prolonged exposure to highly medicalised environments.
Requiring all midwives to begin their careers in obstetric labour wards risks reinforcing the misconception that obstetric care is the default model of birth, rather than one pathway within maternity care.
A more balanced system would allow midwives to develop expertise along different clinical pathways, depending on where their skills and interests lie.
Two Distinct Skill Pathways in Maternity Care?

Over time, midwives naturally develop different areas of expertise depending on where they practise
- this is happening already….
Labour Ward and Obstetric Practice

Midwives working primarily on labour wards already become highly skilled in:
CTG interpretation
medication protocols and drug dosages
epidural care
supporting obstetric interventions
managing emergencies in multidisciplinary environments
These are essential skills for women who choose obstetric care.
Labour wards are built around rapid escalation,
where additional clinicians and equipment are immediately available.
Continuity and Physiological Birth Practice

Midwives working in continuity models or home birth teams develop a different but equally specialised skill set.
These include expertise in:
supporting physiological labour
recognising early signs that labour is deviating from normal
neonatal resuscitation in low-technology environments
risk assessment and transfer decision-making
relationship-based care through continuity
These midwives often work autonomously,
without a room full of clinicians available at the press of a buzzer.
This is not a lesser skill set — it is simply a different form of expertise.
Continuity of Care Matters

The very word midwife means “with woman.”
Historically, midwives supported women throughout pregnancy, birth and the postnatal period.
In many modern systems, care has become fragmented into separate tasks — antenatal clinics, labour ward shifts and postnatal visits — meaning midwives rarely see the full journey of the women they support.
This reductionist model makes it harder for professionals to understand the longer-term impact of decisions made during pregnancy and birth.
Continuity models restore relationship-based care. Midwives who follow women through pregnancy, birth and the postnatal period develop deeper understanding of physiology, risk and early signs of deviation.
Evidence consistently shows that midwife-led continuity models improve outcomes and reduce interventions.
Leadership Matters

Where maternity services function well,
strong clinical leadership is usually present.
Experienced Directors of Midwifery and Consultant Midwives often know their teams well and understand:
which midwives are confident attending home births
which midwives prefer labour ward practice
where additional training may be needed
Good leadership allows services to place the right midwives in the right environments.
Where leadership is weak or unstable,
decision-making can become defensive.
Organisations may revert to the assumption that hospital labour wards are always the safest option.
(exactly what we are seeing across England with the homebirth team suspensions)
However, this assumption is not supported by the evidence.
When Skills Are Not Recognised

When maternity services misunderstand the distribution of skills within their workforce, the response can sometimes be to restrict options rather than organise teams more effectively.
For example, services may suspend home birth provision or limit access to birth centres when staffing pressures arise.
Yet these decisions may not reflect the actual competencies of the midwives working within the service.
A workforce may include midwives who are highly experienced in physiological birth and community practice, but without systems to recognise and maintain those skills, services may default to the assumption that hospital labour wards are the safest environment.
In reality, safety depends not simply on location, but on matching the right skills to the right setting.
A Practical Solution: A National Skills Matrix

A national midwifery skills matrix could provide a practical way to recognise and maintain professional expertise.
Rather than relying solely on banding structures,
a matrix would allow maternity services to understand the real distribution of clinical skills within their workforce.
Ideally such a framework would be standardised nationally, through collaboration between NHS England,
the Nursing and Midwifery Council and professional bodies.
This would create consistent expectations across services and provide greater transparency for both professionals and service users.
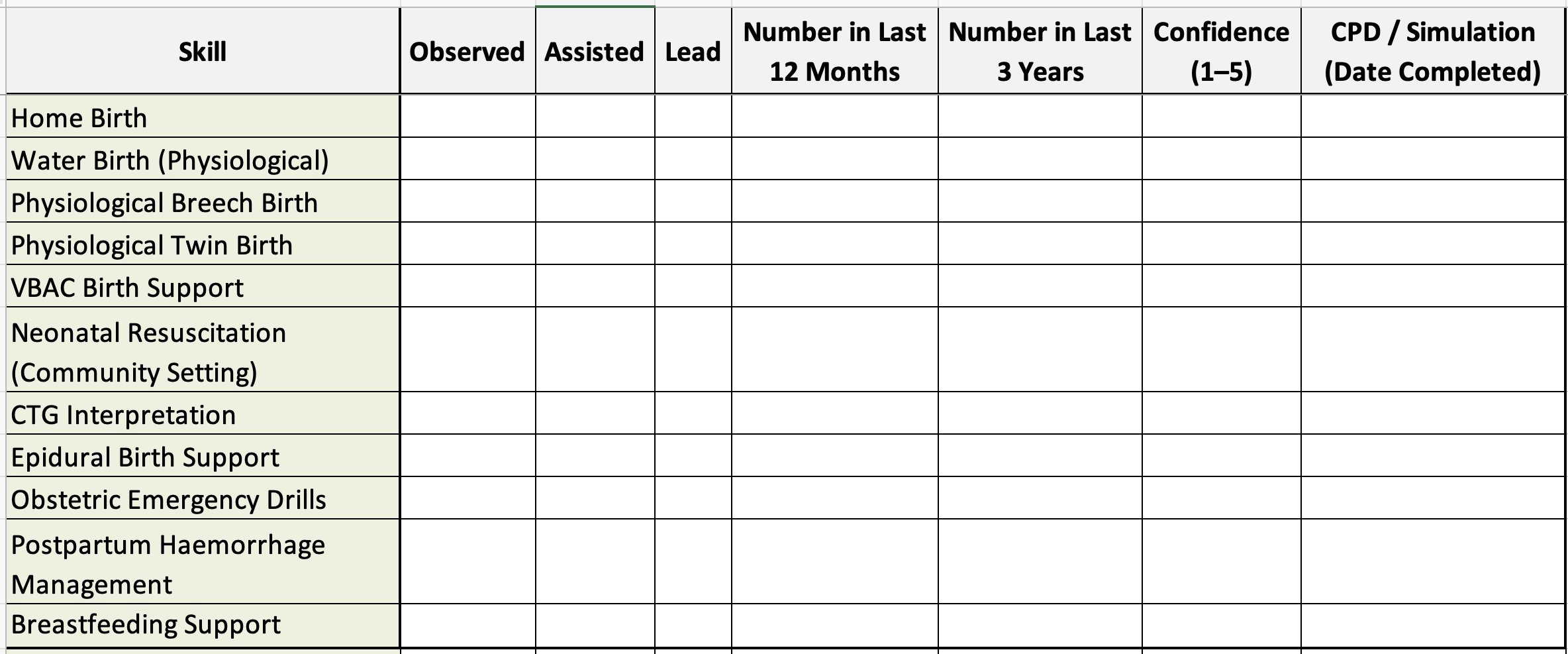
Example Midwifery Skills Matrix
(Annual review model)
A Way Forward

A maternity system that treats midwives as interchangeable units will always struggle to provide safe and responsive care.
Midwives develop expertise through experience.
Some become highly skilled in obstetric environments.
Others develop deep expertise in physiological birth and continuity care.
Both roles are essential.
What is missing in many services is not commitment or professionalism,
but structures that recognise and maintain these different skill sets.
A national skills matrix could help maternity services better understand their workforce, support professional confidence and strengthen continuity models.
Most importantly, it would move the conversation about maternity safety away from assumptions about location and towards what truly matters:
Ensuring the right skills are present in the right environment at the right time.
I would love to hear what you think below…
And while you are here - please consider joining Gloucestershire Maternity Action Group as a member to have your voice fully represented & help us to continue advocating for Gold Standard, Woman Centred, Evidence Based Maternity Care - here in Gloucestershire and across the UK.
